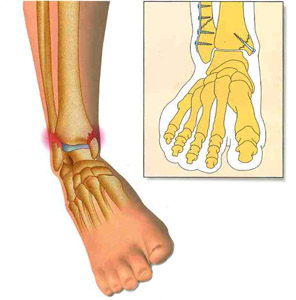
Fractures and dislocations
In the ankle, it is primarily a fracture of the lateral malleolus (same mechanism as the sprain), often not displaced fracture.
Treatments: immobilization by resin’s cast or a walking boot for 1.5 months, with no support prescription of an anticoagulant treatment. If bone fragment displacement or joint involvement: surgical fixation (osteosynthesis).
The other fractures are due to increasing severity: bimalleolar (internal malleolus in addition), trimalleolar (posterior malleolus in addition), tibial pilon (middle of the tibial joint, with great risk of secondary osteoarthritis).
At the level of the foot we find various fractures that can interest all the bones of the foot (usually falling object, jumping reception or torsion) with 2 particularities:
Fracture of the calcaneum (lesion by fall of height on heel or breakage, consolidation time of up to 3 months)
Fracture of the base of the 5th metatarsal (same mechanism as the ankle sprain), very classic
At the foot level, in addition to these classical fractures, “stress fracture” can be found. They occur preferentially during repeated microtrauma (jogging, hiking, etc.).
They concern in order of frequency: the metatarsals, the navicular (internal bone of the middle foot in the jumper in height), the calcaneum, the sesamoids (small bones located at the base of the big toe, plantar face). These fractures are often micro-crack or not displaced, not visible on simple x-rays, requiring diagnosis by a scanner or most often MRI.
Example at the 5th metatarsal: displaced fracture requiring surgical fixation (osteosynthesis)

At the level of the toes: fracture and dislocation. Treatment: reduction + strapping (syndactyly), and walking with a shoe with heel support.
Toe sprain: immobilization 10-15 days by strapping with 2 contiguous toes (syndactyly) then recovery of early mobility by self-reducation

