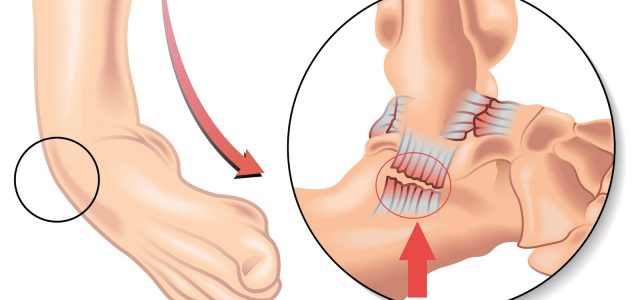
Sprains of the ankle
It occurs in the external lateral ligament of the ankle in 90% of cases.
They are the most common of all traumatic lesions (because the ankle is easily ‘unbalanced’). Unfortunately, these are the most poorly treated lesions.
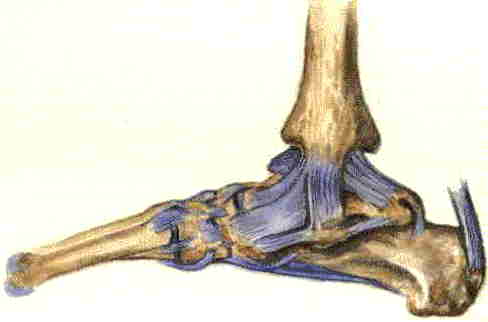
A sprain is a ligament tear. Ligament is a tissue that connects two or more bones to each other, ensuring the stability of a joint.
So that, ankle sprains can be severe with a complete ligament rupture, or benign with a partial tear of these ligaments.
First, it is essential in case of sprain to deflate the ankle. To do this one must raise the foot in relation to the knee, like the gravity of Newton on the one hand. On the other hand, the ankle should be frozen (not directly in contact of the skin with an interposition fabric, such as a dishcloth or towel).
Different types of ankle sprains
There are 4 types of ankle and foot sprains.
The most classic is the sprain of the external lateral ligament that occurs when the foot is twisted inwards. There may be a cracking, then swelling (edema), and often an external hematoma (“pigeon egg”). It imposes the immediate stopping of the sport frequently, and sometimes an impossibility to put the foot on the ground.
Another type is the sprain of the internal lateral ligament (reverse movement of the external ligament, foot towards the outside).
There are also sprains in the middle foot. These sprains require immobilization in a walking boot:
- Chopard’s sprain (spacing between talar bone and tarsus bone (mid-foot bone)),
- Lisfranc’s sprain (spacing between bones of tarsus and metatarsals bones).
Ankle sprains are immobilized by orthotics blocking the movement of the foot inwards or outwards, orthotics that consist of 2 rigid parts on either side of the ankle, connected by “scratches”. Concerning the sprains of the middle foot, these require a walking boot, in order to block any twisting of the middle of the foot.
Therapeutic management
Initially we have to stop its activities, we froze and raises the ankle. Crutches are necessary in case of impossibility to place the foot on the ground.
The ankle is immobilized in a resin splint for a total of 6 weeks. The splint or orthosis consists of 2 semi-rigid valves connected by scratches to wear 3 weeks day and night, then 3 weeks day only. This splint will prevent any movement of the ankle inward or outward.
We supplement with painkillers, anti-inflammatories, cryotherapy (frosting), and specific proprioceptive rehabilitation (for about 1 month ).
Otherwise you risk repeated sprains with chronic instability, which can lead to Surgery (ligamentoplasty). In the case of a resin boot, with the impossibility of placing the foot on the ground, an anticoagulant treatment will be prescribed.
Overall, it takes 45 days for ligament healing. Thus an ankle sprain requires immobilization blocking any movement during this period. “the fact you’re painless, doesn’t mean the ligament is healed”. It can be allowed after 3 weeks of wearing the brace or orthotic day and night, and only wear it during the day, when the patient is in charge.
Two points are therefore essential to prevent recurrence for minimal trauma: respect this healing time of 45 days, and work on proprioception.
Proprioception is the act of stimulating the nerve endings of the sole of the foot to the support to prevent the risk of recurrence. It is given for this in addition to the physiotherapy sessions. This consists of self-rehabilitation and rolling a tennis ball or baseball under the foot, and a small bottle of frozen water of 50 cL under the foot for 5 minutes several times a day. In this way, mechanoreceptors and thermoreceptors can be stimulated.
The rest of the treatment also includes rehabilitation sessions (started 10 to 15 days after the initial trauma). The main objective of rehabilitation is the recovery of joint amplitudes. There may also be a proprioceptive work complement. This may also be a prescription for orthopaedic soles.
Chronic instability
Chronic instability is reported in the following situations: the ankle no longer holds its foot to walking on soft, sandy or uneven ground; the occurrence of sprains occurs frequently, for minimal trauma, or interferes with sports activities. It can also occur through chronic swelling of the ankle, blockages, or pain in localization, and may be complicated by long-term osteoarthritis due to repeated cartilage shocks.
Ligament hyperlaxity, neurological disorders and balance, triceps or Achilles tendon pathology, internal deflection of the ankle axis will be investigated. Standard x-rays, as well as comparative x-rays of the two ankles to the inside and the outside, will be performed, supplemented by an MRI or arthro-scanner.
In cases of chronic instability resistant to medical treatment, there may therefore be a surgical indication. We can then propose a stabilization of the ankle by Ligamentoplasty. This involves using a fibular tendon to strengthen or reconstruct the ligament plane. A walking boot should be worn for 6 weeks, with no support (crutches and anticoagulants) for the first 3 weeks.
The management of ankle sprains is important… Too many patients have neglected their healing. It is not because the ankle is not painful that it is “consolidated”. It can drag on for years, and you can have multi-year recurrences for minimal trauma…